
OpenAI o3 Helped Experts Revisit 376 Unsolved Rare-Disease Cases
A study published in NEJM AI on June 18, 2026 used OpenAI o3 Deep Research to reanalyze 376 rare-disease cases that had remained unsolved after earlier specialist review.
The result was not autonomous diagnosis. The model generated evidence-linked hypotheses that physicians and genetic experts investigated through established clinical processes.
After expert review, additional testing, variant classification, laboratory confirmation, and communication through clinical teams, 18 cases received diagnoses. That represents a reported 4.8% additional diagnostic yield in a population whose cases had already resisted earlier analysis.
What the OpenAI o3 Rare Disease Study Actually Tested
The OpenAI o3 rare disease study evaluated whether a general-purpose reasoning model could help specialists revisit difficult genetic cases.
Researchers from Boston Children’s Hospital’s Manton Center for Orphan Disease Research, Harvard University, and OpenAI assembled de-identified case packets containing clinical features, age and sex metadata, family information, and filtered genomic variant tables. Clinical features were standardized using Human Phenotype Ontology terms.
The model was asked to propose the most plausible molecular explanation and support that hypothesis with reasoning connecting:
- The patient’s clinical features
- Inheritance patterns
- Variant rarity
- Predicted biological effects
- ClinVar classifications
- Family sequencing evidence
- Relevant scientific literature
The output was not accepted as a diagnosis. It functioned as a structured hypothesis for specialists to examine.
How the Human-Guided Workflow Worked
The study used a multi-stage review process.
First, OpenAI o3 analyzed the de-identified case material and proposed candidate explanations.
Second, at least two experts reviewed each candidate using the ACMG/AMP framework used by clinical laboratories to classify genetic variants.
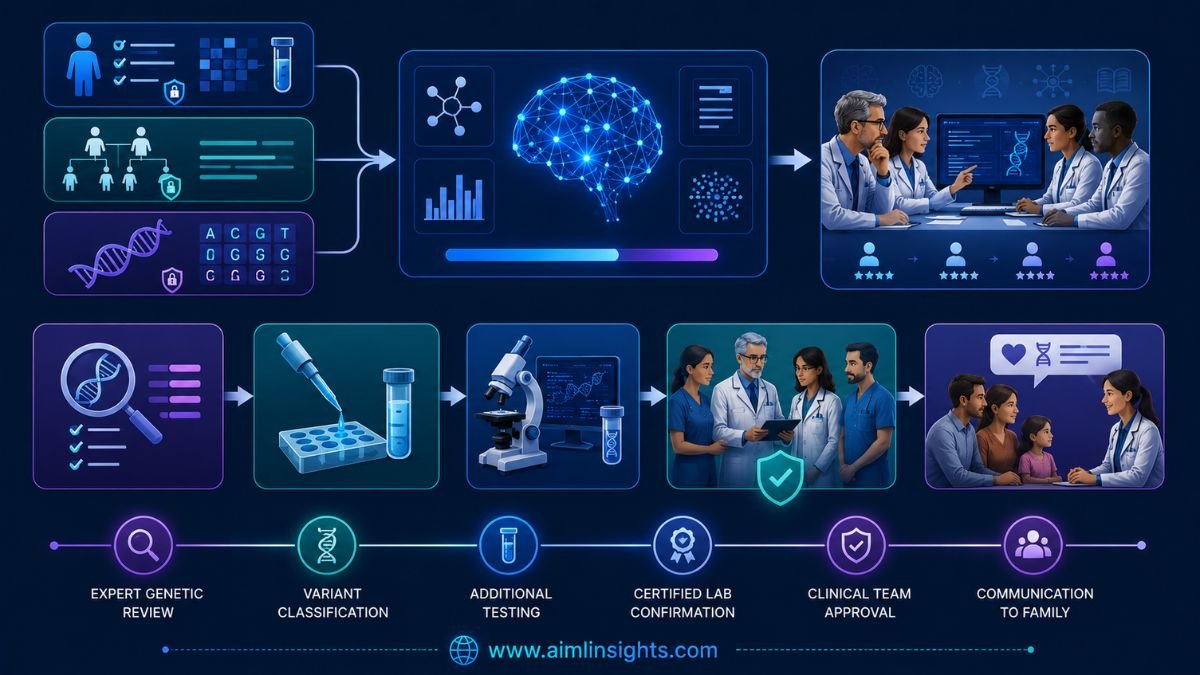
Third, disagreements were resolved through expert consensus.
Fourth, a case counted as diagnosed only when the variant was considered pathogenic or likely pathogenic, a certified clinical laboratory confirmed the finding, and the result was returned through the clinical team.
The workflow can be summarized as:
Clinical and genomic data → AI-generated hypothesis → expert review → follow-up testing → laboratory confirmation → clinical communication
This is decision support. The model widened the search space and helped prioritize evidence. Qualified clinicians retained responsibility for interpretation and diagnosis.
What the Researchers Found
The 376 cases came from four different groups:
| Cohort | Cases | Confirmed diagnoses | Reported yield |
| Neurodevelopmental conditions | 100 | 10 | 10.0% |
| Neuromuscular disease | 61 | 4 | 6.6% |
| Sudden unexpected death in pediatrics | 200 | 2 | 1.0% |
| Early psychosis | 15 | 2 | 13.3% |
| Total | 376 | 18 | 4.8% |
The early-psychosis group was very small, so its 13.3% figure should not be interpreted as a stable estimate for that population. Diagnostic yield also differed because the cohorts varied in how likely they were to have a single-gene explanation.
Seven of the 18 diagnoses were rediscoveries. Those diagnoses had been established elsewhere but were absent from the local records reviewed in the study. This suggests that some value came from connecting fragmented information rather than discovering entirely new biological explanations.
Why Previously Unsolved Cases Can Become Solvable
A negative genetic result can become outdated.
The patient’s genome may not change, but scientific knowledge does. Researchers continue to identify new gene-disease relationships, reclassify variants, publish case reports, and improve understanding of inheritance and phenotype patterns.
A case that was uninterpretable several years ago may become diagnosable when new evidence appears.
The difficulty is scale. Rare-disease teams may need to revisit thousands of cases while tracking changing literature, updated databases, clinical records, family data, and variant annotations. The study tested whether a reasoning model could help specialists synthesize that evolving evidence more efficiently.
What Was Genuinely New
The model did more than rank candidate genes.
It was asked to produce an explanation that connected the phenotype, family inheritance, genomic evidence, and literature into a reviewable argument.
In one early-psychosis case, the model inferred a possible chromosome 22 structural event from a pattern of low-quality genomic calls and the patient’s cardiac, immune, neurodevelopmental, and psychiatric features. Follow-up genome sequencing confirmed a 22q11.2 deletion associated with DiGeorge syndrome.
In other cases, the model proposed that two genes together might explain a complex presentation, rather than forcing all symptoms into one monogenic diagnosis. It also generated possible biological hypotheses that remain unconfirmed and require experimental validation.
That distinction is important. A useful research hypothesis is not the same as a clinically confirmed diagnosis.
Study Validation Before the Unsolved Cases
Before applying the workflow to unresolved patients, the researchers tested it on previously solved cases.
The official study summary reports that the workflow recovered the correct gene and variant in duplicate runs for 48 of 51 established cases. In 57 neuromuscular cases, it returned the correct diagnosis in duplicate runs for 45 cases. In a 15-case long-read genome set, it identified the correct gene in every case and both disease-causing alleles in 12.
These evaluations helped refine the prompting and review process, but they were not independent external benchmarks. They were part of the same research program and did not compare o3 directly with another model or a standard human-only reanalysis workflow.
Benchmark Audit: OpenAI o3 Rare Disease Study
| Evaluation | Metric | Reported result | Baseline | Evaluation owner | Independently verified? |
| Previously unsolved cohort | Additional diagnostic yield | 18 of 376 cases, or 4.8% | Earlier specialist analysis had not resolved the cases | Study authors | No independent replication |
| Established mixed cases | Correct gene and variant in duplicate runs | 48 of 51 | Known diagnosis | Study authors | No |
| Neuromuscular validation set | Correct diagnosis in duplicate runs | 45 of 57 | Known diagnosis | Study authors | No |
| Long-read genome set | Correct gene | 15 of 15 | Known diagnosis | Study authors | No |
| Long-read genome set | Both causal alleles | 12 of 15 | Known diagnosis | Study authors | No |
Several details are missing from a full comparative assessment:
- No randomized human-only control arm
- No blinded comparison against standard reanalysis
- No comparison with other AI models
- No systematic false-positive count
- No total number of candidate hypotheses reviewed
- No time or cost measurement
- No clinician-effort measurement
- No assessment of treatment or outcome changes
The 4.8% yield is therefore meaningful but narrow. It shows that expert-led AI-assisted reanalysis surfaced clinically confirmable leads in some difficult cases. It does not show that o3 is a standalone diagnostic system.
Decision Support Is Not Medical Decision-Making
The safest interpretation is that o3 acted as a research assistant.
It could synthesize scattered evidence, propose candidate explanations, and help experts decide what to investigate next.
It could not:
- Establish a diagnosis independently
- Order clinical tests
- Classify a variant on its own
- Decide what result should be returned to a family
- Recommend treatment
- Replace genetic counseling
- Replace certified laboratory confirmation
OpenAI explicitly states that the study is not evidence that patients or clinicians should use ChatGPT, o3 Deep Research, or another OpenAI product to diagnose disease or make medical decisions.
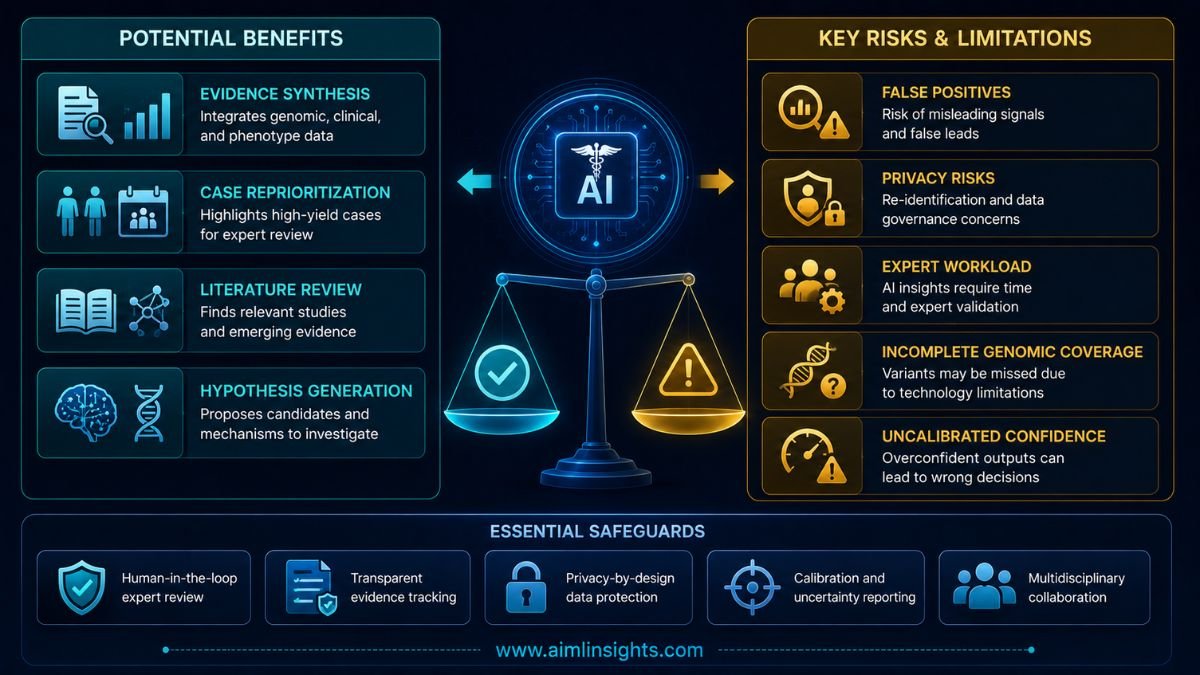
Why This Matters
Rare-disease diagnosis often depends on connecting information spread across different systems.
Clinical notes may use one vocabulary, genomic databases another, and research papers a third. Family histories, structural clues, older test results, and newly published evidence may not be visible in one place.
A model that helps specialists organize and interrogate this material could make periodic reanalysis more practical.
The potential value is not replacing expertise. It is helping experts revisit more cases, generate testable hypotheses, and focus limited time on candidates with coherent supporting evidence.
For families who have waited years for an answer, even a single-digit additional yield may matter. But the benefit must be weighed against false positives, review workload, privacy requirements, and the cost of confirmatory testing.
Privacy and Deployment Requirements
The study used de-identified information and did not transmit protected health information outside approved environments.
Broader clinical use would require strict controls for data access, auditability, security, consent, local regulation, and record retention. It would also require versioned prompts, reference checking, calibrated uncertainty, and clear documentation of how each candidate was generated.
Hospitals would still need sequencing infrastructure, bioinformatics pipelines, clinical geneticists, certified laboratories, and genetic counselors.
The model is only one layer in a much larger clinical system.
Limitations and Unanswered Questions
The study was retrospective and included heterogeneous cohorts.
Reviewers were not blinded to the model’s confidence scores. Those scores tracked with correctness in solved cases, but they were not calibrated probabilities and were not used as substitutes for evidence.
The researchers did not measure:
- Time saved
- Total cost
- False-positive workload
- Number of rejected hypotheses
- Changes in clinical care
- Effects on patient outcomes
- Performance in prospective use
- Performance across multiple hospitals
The study also did not systematically test all forms of genomic variation, including repeat expansions, deep-intronic variants, mosaicism, and some structural variants.
Large language models can also produce plausible but incorrect explanations. That risk is especially serious in medicine because a convincing narrative may encourage unnecessary testing or distract experts from better candidates.
Simple Explanation for Beginners
Imagine a child has years of medical records, genetic test results, family information, and symptoms—but no diagnosis.
OpenAI o3 reviewed a structured, de-identified version of that information and suggested possible genetic explanations.
Doctors and scientists then checked those ideas, ordered more tests when needed, and confirmed some results in certified laboratories.
The AI suggested where to look. The experts decided what was true.
What Comes Next
The most useful next step would be a prospective, multicenter study.
Researchers would need to compare AI-assisted reanalysis with normal practice using the same cases and measure:
- Additional diagnostic yield
- Time to a useful candidate
- Clinician workload
- False-positive burden
- Cost per confirmed diagnosis
- Patient outcomes
- Differences across hospitals and populations
Such work would clarify whether the workflow is practical beyond one expert research setting.
Conclusion: OpenAI o3 Rare Disease Study
The OpenAI o3 rare disease study shows that a general-purpose reasoning model can help specialists revisit difficult genomic cases and generate evidence-linked hypotheses.
Experts ultimately established 18 diagnoses among 376 previously unsolved cases, a reported additional yield of 4.8%.
That is clinically interesting, but it is not evidence of autonomous diagnosis.
The strongest conclusion is more measured: AI may help qualified teams search, connect, and prioritize complex evidence, while medical decisions remain with clinicians, laboratories, and patients.
Final Takeaways
- The study was published in NEJM AI on June 18, 2026.
- Researchers reanalyzed 376 previously unsolved rare-disease cases.
- OpenAI o3 generated evidence-linked molecular hypotheses.
- Specialists reviewed every candidate.
- Follow-up testing and certified laboratory confirmation were required.
- Physicians established 18 diagnoses, a reported 4.8% additional yield.
- Seven diagnoses were rediscoveries missing from the reviewed local record.
- The study was retrospective and had no randomized human-only control group.
- It did not measure cost, time saved, false-positive burden, or patient outcomes.
- The model provided decision support; it did not diagnose patients.
Suggested Read:
- AI Agents Can Now Work for Hours
- China’s Cheap AI Model Is Making Claude Look Expensive
- Latest AI Research News
- Claude Cowork Explained
- AI Cybersecurity Risks Explained
- How RAG Systems Work
FAQ: OpenAI o3 Rare Disease Study
What did the OpenAI o3 rare disease study find?
The study found that an expert-led workflow using OpenAI o3 helped surface clinically reviewable leads that resulted in 18 confirmed diagnoses among 376 previously unsolved cases.
Did OpenAI o3 diagnose 18 patients?
No. The model generated hypotheses. Qualified specialists reviewed the evidence, follow-up tests were performed, and certified laboratories confirmed the findings before physicians established diagnoses.
How was o3 used in genomic reanalysis?
It analyzed de-identified phenotype information, family data, filtered genomic variants, database annotations, and scientific literature to propose molecular explanations for expert review.
What does 4.8% additional diagnostic yield mean?
It means 18 of the 376 previously unresolved cases received diagnoses after the AI-assisted expert reanalysis process. It does not mean the model independently diagnosed 4.8% of patients.
What were the limitations of the study?
It was retrospective, lacked a randomized human-only comparison, did not measure cost or time saved, and did not systematically test every form of genomic variation.
Can patients use ChatGPT to diagnose a rare disease?
No. OpenAI states that the study does not support using ChatGPT or o3 for diagnosis or medical decision-making. Patients should work with qualified healthcare and genetics professionals.
References: